EG.5 is a family of Omicron variants (descended from XBB.1.9.2) that first appeared back in February 2023.
The World Health Organization (WHO) classified it as a “variant under monitoring” on July 19 after a surge in COVID infections from early July. It has been increasingly reported across the globe, particularly in Asia.
On August 9 2023, it was upgraded to a “variant of interest”. This follows the rise of a particular variant, EG.5.1, known as Eris. But it has not been classified a “variant of concern”.
Eris has seen EG.5 jump from 7.6% of all SARS-CoV-2 genetically sequenced globally in late June, to 17.4% in the week of July 17-23.
Eris has edged out other Omicron variants circulating in the United States, and now makes up the largest proportion of COVID cases there.
But while it has been in Australia since April, cases have remained sporadic.
Is Eris different to other variants?
At this stage, there is no evidence EG.5.1 causes more severe disease than other Omicron variants, and it seems to cause similar symptoms.
How this virus enters cells and tissues in our body is also similar to XBB.1.5 (sometimes referred to as Kraken) and other Omicron variants.
While the severity of the illness it causes will need to be documented carefully, there are no indications it’s different from XBB.1.5.
The virus has changed, incrementally, making EG.5.1 more transmissible. While this enables it to compete with other circulating variants, it’s unclear if or when Eris will out-compete other variants in Australia.
What variants is the WHO watching?
The WHO defines a variant of interest as one that has genetic changes that could increase its transmissibility, virulence, its ability to evade vaccines, be treated with drugs or detected via current testing methods – as well as already demonstrating a “growth advantage” over other circulating variants.
The current variant of interest list also includes two other Omicron cousins – XBB 1.5 and XBB 1.16 (the latter sometimes referred to as Arcturus). Both have been circulating in Australia since the start of the year.
Yet, another XBB variant that has been around since February and dominated over our autumn-winter peak in Australia, XBB 1.9, has remained on the WHO’s lesser “variants under monitoring” list.
This shows a variant’s transmission advantage in a particular region depends on a range of factors, including waning immunity given the time lag since the last wave, vaccine booster timing, and coming into cooler weather.
How closely related the new variant is to the variants already circulating in the population is another key factor. The more different it is, the less likely it is our immune system to will recognise it quickly and be able to fight off infection.
Will vaccines protect against it?

Current vaccines still offer protection. Unsplash/CDC
EG.5.1 has two important additional mutations that XBB.1.9.2 does not have: F456L and Q52H, whereas EG.5 only has F456L. The extra small change in EG.5.1, the Q52H mutation in the spike protein, is enough to give EG.5.1 an edge over EG.5 in transmissibility.
The good news is the bivalent vaccine antibody responses to EG.5.1 are similar to those for variants that dominated earlier in the year in Australia.
In research yet to be published (and peer reviewed) from my team at the Kirby Institute, we isolated and characterised EG.5.1 and compared it with other circulating variants in Australia. We found that while the antibody response wanes the longer it has been since the last vaccine dose or infection, this is not at levels significantly different to XBB.1.5.
Importantly, bivalent vaccine doses, such as Moderna’s BA.1 bivalent booster, generate a five-fold increase in antibodies that protect against variants in circulation, including EG.5.1.
Will Eris prompt a rise in COVID cases?
EG.5.1 has been in Australia since April and it’s still only appearing sporadically. By August 7 2023, there had been 158 known cases reported via whole genome sequencing across Australia, representing 2.1% of reported variants.
Encouragingly, Australia’s overall infection rates continue to decline, as do hospitalisations and COVID-related deaths, antiviral scripts, and reports of cases in aged care.
While Australia may simply be lagging behind the US, we may see a different pattern entirely.
India first saw this variant back in May, but it has also seen only sporadic cases, and no major rise in overall infections. Like Australia, it is the XBB family of Omicron variant that continue to dominate in India, accounting for 90-92% of infections.
Given the ancestral variant for EG.5.1 is XBB 1.9, which was our dominant variant over winter, it’s also possible we might have better population level immunity than countries like the US. As we start to emerge from our winter, with boosted natural immunity and booster vaccination, we may be less likely to see this EG.5.1 muscle out other variants.
However, as our immunity wanes, with greater distance since our last wave, we will inevitably see infection rates start to push up again – potentially in late spring. EG.5.1 might drive this, or it could be another variant currently circulating.
COVID is becoming less of a threat but still needs watching
It’s reassuring that the intervals between COVID waves in Australia are increasing and the heights of the peaks are diminishing with each successive wave since Omicron arrived.
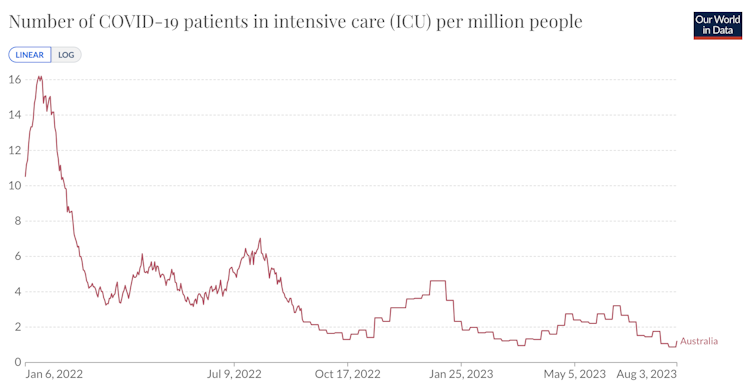
The number of Australian COVID-positive patients admitted to ICU over the Omicron waves. Our World In Data, CC BY
It’s also heartening that emerging variants aren’t genetically that different, so our immunity, vaccines, testing and treatment are still effective in protecting us from serious illness.
Time is our ally. The more time our immune systems have to mature, the more they can respond to a range variants far better than before. Our antibodies may wane over time, but the pool that are left represent quality rather than quantity in their ability to target many variants.
The virus is changing, with Omicron variants gradually taking over from others. But we need to remain vigilant and keep minimising infection risk where we can, and monitoring the genomic data so we’re alert to any seismic shifts and take note if a variant is classified as a variant of concern.

Catherine Bennett, Chair in Epidemiology, Deakin University and Stuart Turville, Associate Professor, Immunovirology and Pathogenesis Program, Kirby Institute, UNSW Sydney
This article is republished from The Conversation under a Creative Commons license. Read the original article.